Guiding healthy growth, breathing and sleep, at any age.
At Growth and Airway, we take a fundamentally different view of dental and craniofacial health. Conventional care tends to treat problems as they present: jaw pain managed with a night splint, crooked teeth corrected with braces, sleep apnoea managed with a CPAP machine. We ask what created those problems in the first place.
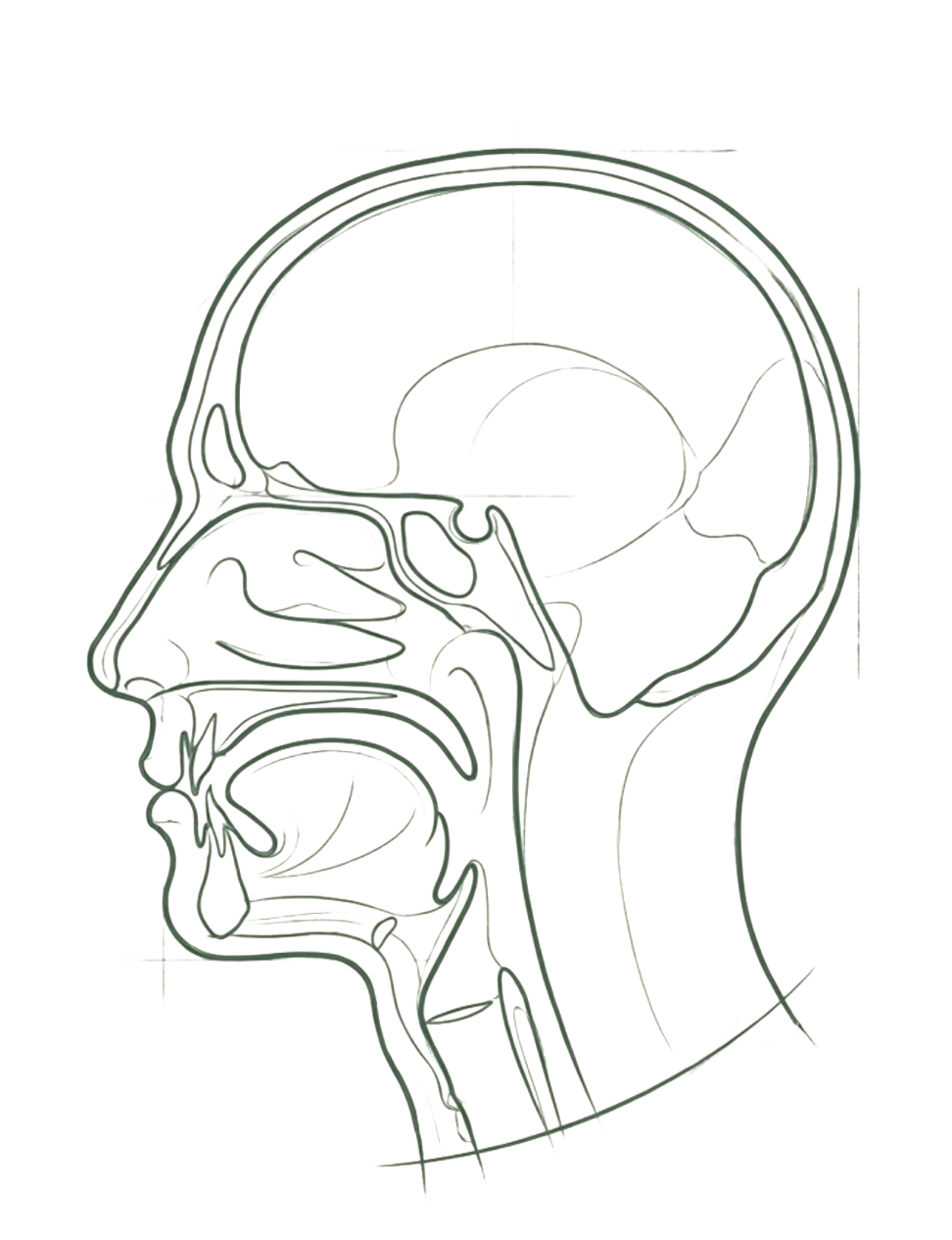
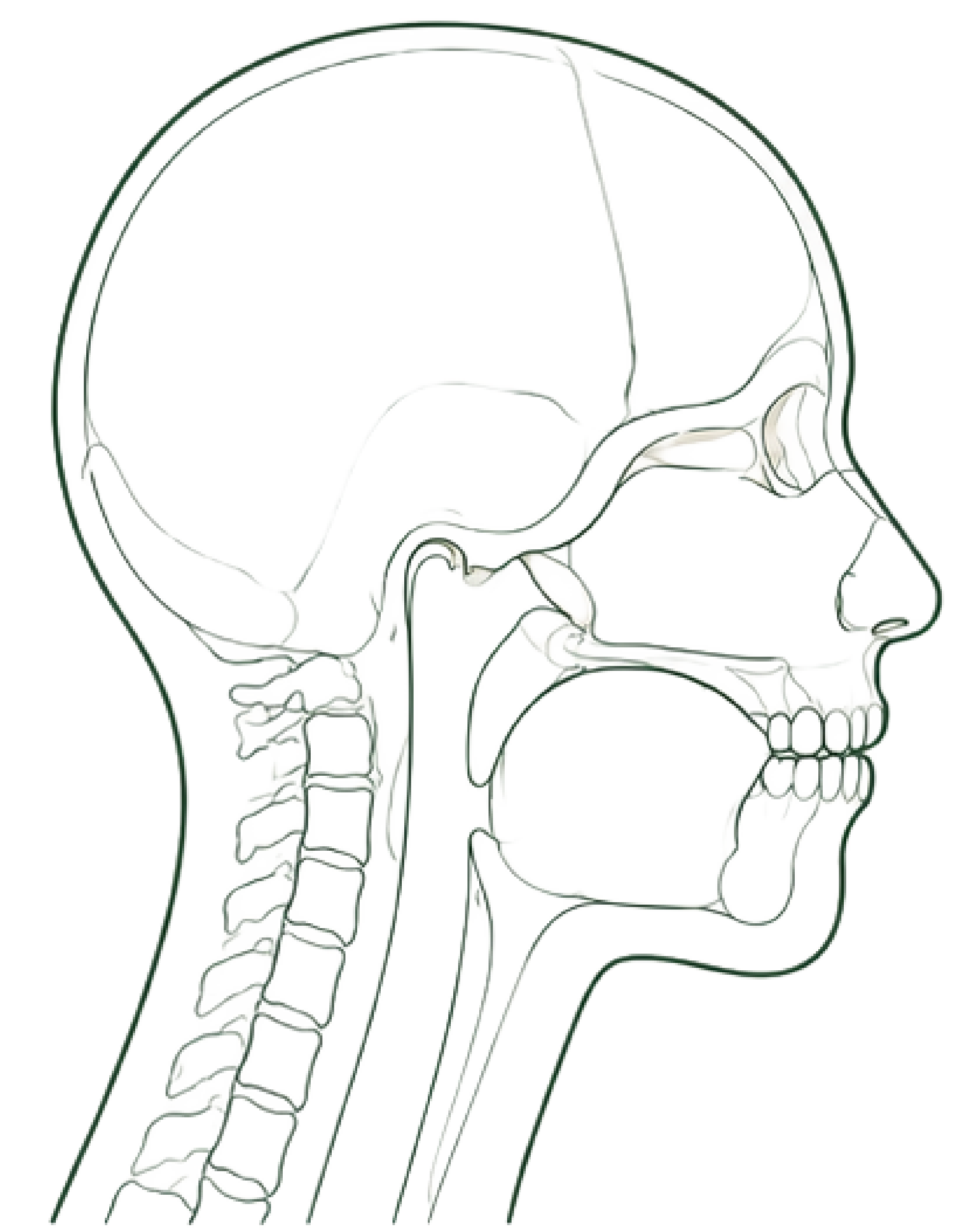
In the majority of cases, the answer lies in the development of the jaws, the airway, and the soft tissues that govern how we breathe, swallow, and rest. TMJ pain, bruxism and teeth grinding, mouth breathing, tongue tie, and sleep-disordered breathing are not separate and unrelated problems. They share common structural roots. When those roots are properly addressed, meaningful and lasting change becomes possible.
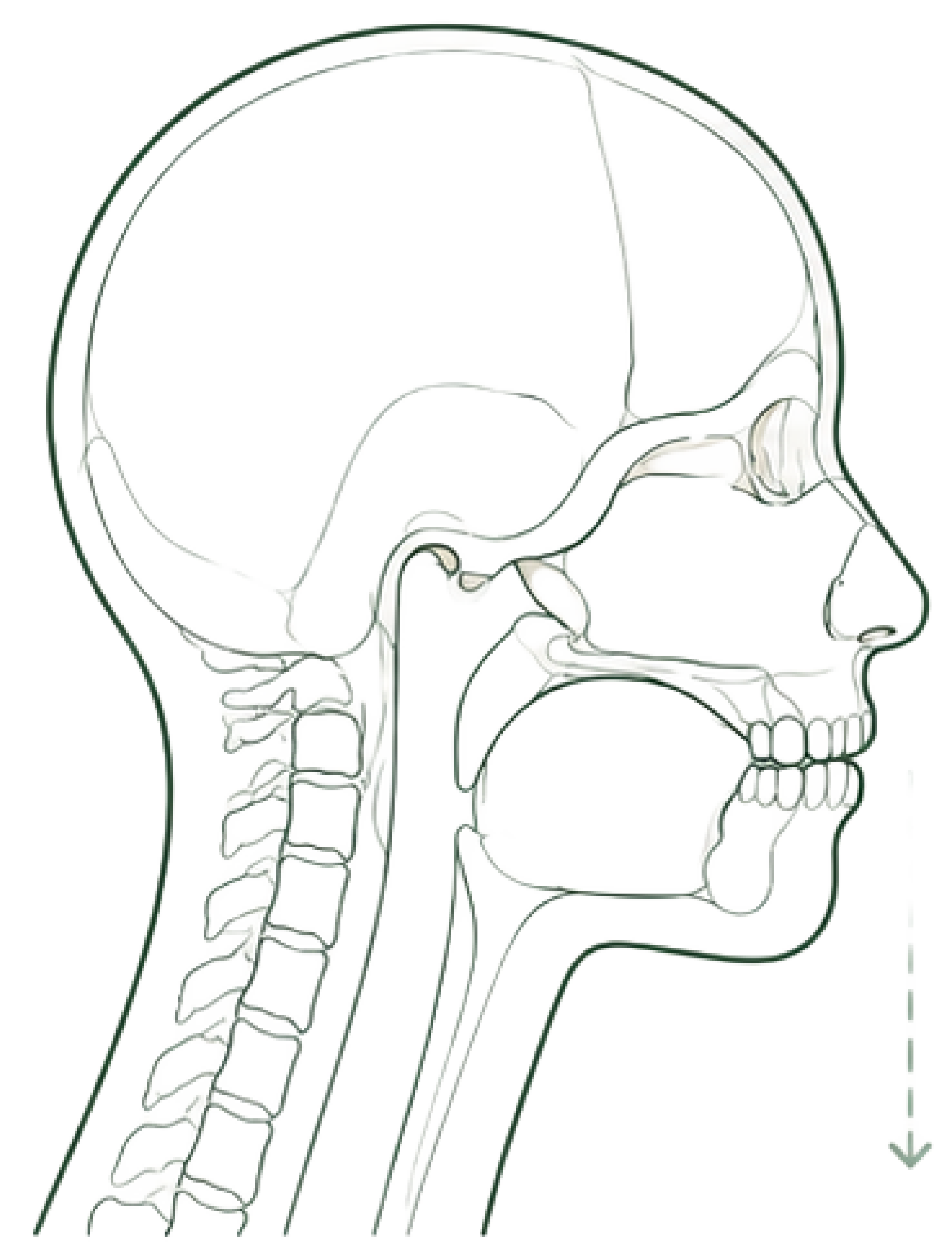
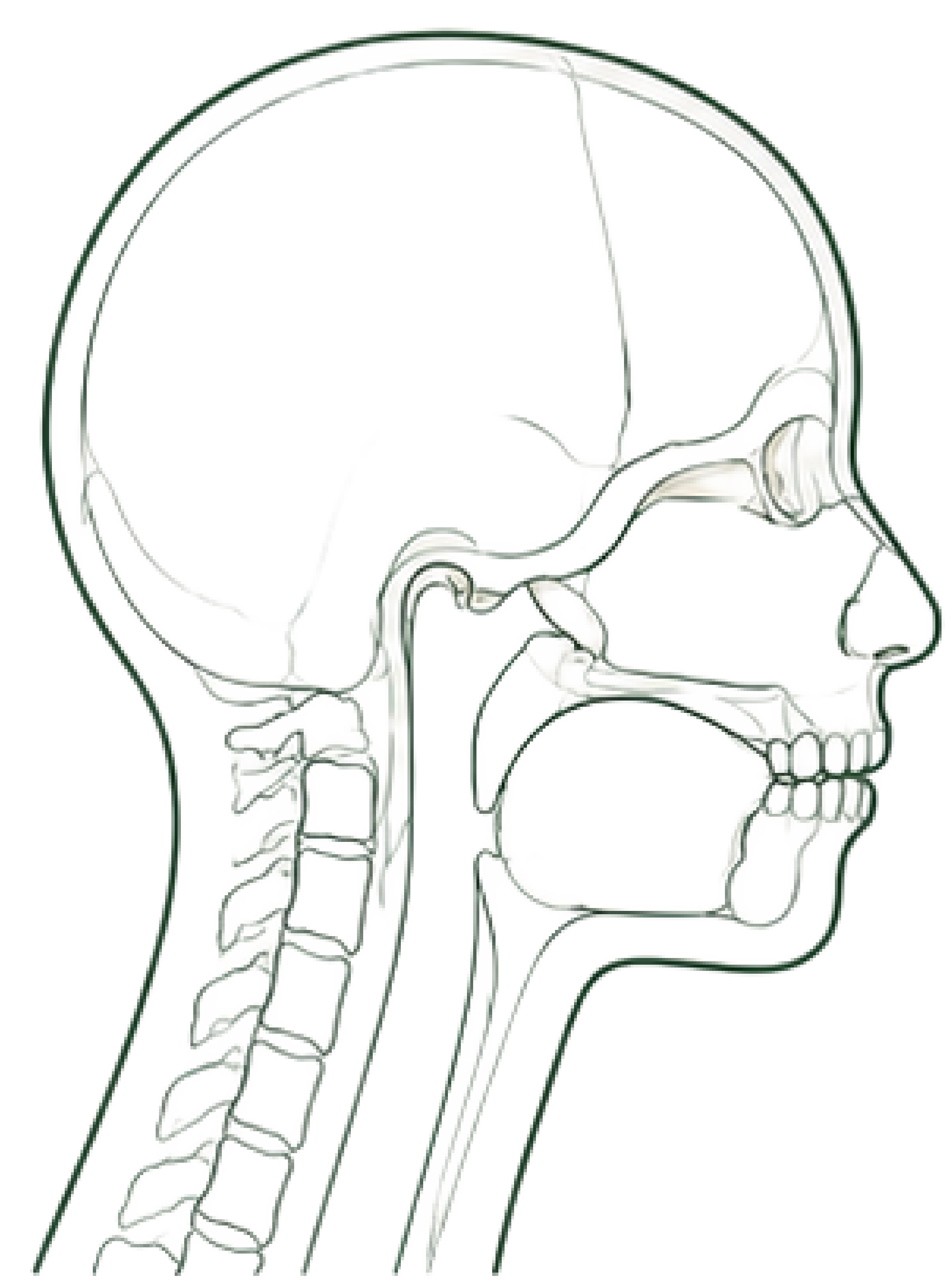
We work across the full lifespan. For children, we intervene early, guiding craniofacial growth while the face and jaws are still developing and preventing orthodontic and airway problems from becoming entrenched. For adults, we identify and treat the underlying structural causes of TMJ disorder, sleep apnoea, bruxism, and related conditions rather than simply managing symptoms over time.